
Infant Feeding Problems
General Discussion
Feeding problems during the first 3 months can be difficult to assess and health professionals similarly will find this area confusing. As with most things in medicine, careful history and examination usually will provide enough clues and there is rarely any need for tests.
A word on irritability. There are lots of theories on why some infants are ‘perfect’ and other infants appear to fuss, cry, and appear distressed. Many theories suggest a gastrointestinal problem but if their are no specific symptoms, such as excessive vomiting, difficulty feeding, diarrhoea, poor weight gain, then it is unlikely that irritability is related to a feeding issue. So feeding related problems can be approached in a logical fashion to help establish the cause and keeping things simple.
- Is there a problem with the amount of milk

- Is there a problem getting the milk into the infant
- Is there a problem digesting the milk
- Is there a problem expelling the waste products
Symptoms such as crying, pulling off the breast, irritability, inconsistent or distressing bowel actions, regurgitation, vomiting, night waking, at times can be part an parcel of a normal infant’s behaviour. But when these symptoms persist for long periods, and there appears to be no let up, it can be very disheartening for parents who will troll the internet looking for answers. The most important issue from a medical point of view is weight gain. If this is adequate then a significant medical issue is unlikely. If weight gain is poor then this needs to be more carefully assessed. So we’ll start with one of the most common infant feeding problems, that results in poor weight gain.
Is there a problem with the amount of milk
This is the most common cause for poor growth in an infant. If the weight gain is poor, the infant appears scrawny, is constantly irritable due to hunger, is trying to feed every hour or so, and expressing after feeding yields very little milk then not enough milk is the most likely issue. This usually presents in the first few weeks, and is one of the reasons why it is important for an accurate weight to be done when assessing infants. The medical term for poor weight gain is ‘failure to thrive’. The most common cause is milk supply, but sometimes infant medical problems will need to be considered. Sometimes it is necessary to ‘buy some time’ by complementary feeding with stored breast milk or formula, whilst addressing factors that have resulted in poor milk supply. Some Mothers will feel like they have somehow ‘failed’ which is simply not true. Many well meaning midwifes will place a great deal of pressure on new Mothers who will feel guilty and upset if they do not provide enough milk. Some breasts just are not cut out for producing milk. The stress of an underfed infant is greater than any benefit from exclusively breast feeding.
Is there a problem getting the milk into the infant?
Next on the list are feeding related problems, usually due to factors that are best diagnosed by a lactation consultant. Problems with the nipples, attachment and suck may well be the cause of feeding related issues. Sometimes infants have an anatomical problem with the oropharyngeal area such as severe tongue tie, soft palate problems, or swallowing issues. Usually the symptoms are obvious and will occur within the first few days of birth.
Is there a problem digesting the milk?
The infant is receiving enough milk, there is plenty of it but there is a problem once inside. I will start by discussing reflux then GORD and finally food protein intolerance
Reflux
Reflux or regurgitation is common in normal healthy infants. Immaturity of the valve at the lower end of the eosophagus results in milk easily going down and then coming back up. Sometimes there are so many episodes Mother’s are amazed the infant is gaining weight. There are no other distressing symptoms and are growing, have normal bowel actions, are happy to feed and the symptoms do not really bother them. There is no real need to take any action apart from elevating the cot. Many paediatricians call these infants “happy chuckers”. They will often slightly worsen as they become more mobile between 4 – 6 months of age. Some will still ‘chuck’ until 12 months or so.
Gastroeosphageal Reflux Disease
This is a controversial condition that was probably overdiagnosed during the 80s and 90s. It is not as common as people believe despite the fact that many infants are placed on reflux medication, often unnecessarily. True reflux disease involves poor weight gain, problems feeding, with difficulty swallowing, frequent vomiting and possetting, and sometimes problems with the upper airways. Note that these symptoms are very similar to food protein intolerance and what used to be called severe reflux was possibly severe food protein intolerance. Many paediatricians feel pressured to treat for GORD as it is commonly diagnosed by Google, allied health professionals and well meaning relatives and parents feel pressured to ‘do something’. What makes this difficult is that there are no simple tests to help diagnose GORD.
Silent reflux is a term that is popular on the internet but probably does not really exist. The symptoms describe an irritable infant who does not posset or reflux much, hence the ‘silence’. Desperate parents will often find this on the internet and request reflux treatment. There is little evidence for this condition and treatment is disappointing.
Food Protein Intolerance
Bit of background. Protein, carbohydrate and fats represent the major nutritional requirements. They are often called macro-nutrients. Micro-nutrients include vitamins and minerals. Proteins are composed of amino acids, and come in all shapes and sizes. Most protein is ingested in the form of meat, dairy products, and soy. These proteins are passed through the breast milk.
Some proteins appear to cause gastrointestinal distress in some infants. This is different from an allergic reaction, as there is no immune system involvement. So no rash, respiratory distress or features of an immediate obvious reaction. These infants do not enjoy feeding. They appear fussy at the breast, take significantly longer to feed and their growth is ‘just ok’. They have day and night time feed related problems. Some will posset a great deal and some will have inconsistent bowel actions. Unfortunately there are no tests possible and the diagnosis involves maternal dietary restriction. The usual culprits are Cows milk protein, Soy protein and other animal proteins such as Goat. The advice from paediatric gastroenterologists is to try dairy free diet first and only restrict other proteins if there are ongoing symptoms. Many of these infants will grow out of this by the age of 12 to 18 months.
This condition becomes more complicated if formula feeding as most are made from cow’s milk protein. So if changing formulas then moving to a soy based formula is recommended if greater than 6 months. In some instances Goats milk formula is also tolerated. If there is intolerance to soy and cow’s milk protein then specialized formulas that have all the proteins ‘chopped up’ might be needed. In Australia the only over the counter ‘extensively hydrolysed’ formula is allerpro from nutricia. Other fomulas require specialist scripts from paediatric gastroenterologists.
Here is a table of formulas which is more based on allergy than intolerance, but some of the principles are the same.
TABLE OF FORMULAS.
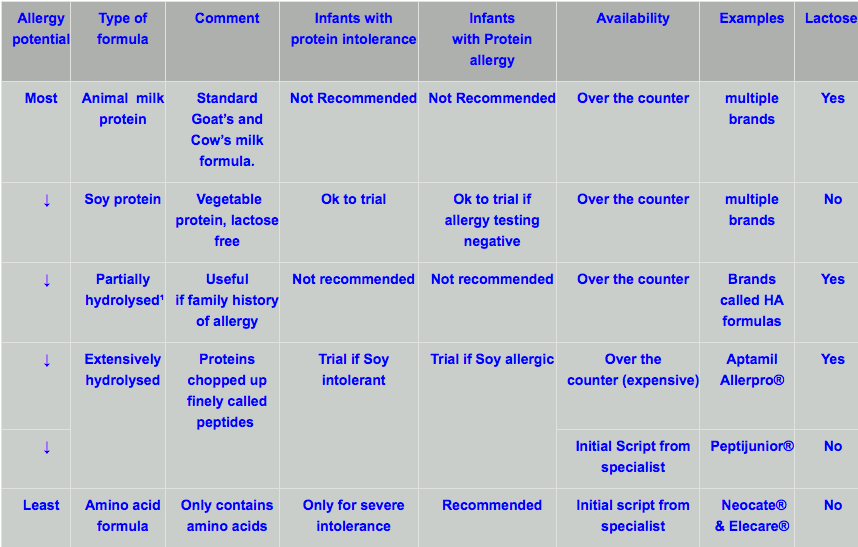
¹ Hydrolysed means the proteins are chopped up.
Is there a problem expelling the waste products ?
Food enters the large intestine after having most of the nutrients removed. The waste products, combined with gastrointestinal bacteria, and some bile pigment make up the colour and consistency of the bowel actions. Sometimes food stuffs are not properly digested by the small intestine and they are fermented by bacteria. This can cause some excess gas and organic acids resulting in bowel distension, bowel actions that can be explosive and similar to diarrhoea and discomfort. Probably what adults would call indigestion.
So some infants will appear ‘bowel centric’ with their irritability. They are healthy, feed well but appear distressed until they pass a bowel action or excess wind. As they get older much of this behaviour settles.
What to do.
If you feel this is useful then perhaps show your doctor. General Practitioners are good at diagnosing a significant medical problem in an infant, but feeding problems are much harder to understand and require expertise that may be beyond your GP. Note the above is a guide, and there are always exceptions to the rules, but these are rare.


